All summer, we at Ascendient have been following the process for creating the North Carolina 2026 State Medical Facilities Plan (SMFP). As the autumnal equinox approaches and the plan reaches finalization, we see some trends that are worth noting – alongside a few surprises.
Following recent State Health Coordinating Council (SHCC) standing committee meetings, we have a clearer picture of what is ahead. While the full Council won’t meet until Oct. 1, committee decisions provide important insights for healthcare organizations conducting comprehensive healthcare planning.
Historic Bed Needs Are Coming
Despite data discrepancies and updates throughout the summer, one thing is clear: the 2026 SMFP will include significant – even historic – acute care bed needs. “I can’t remember a higher total bed need since at least 1990,” says Dawn Carter, Ascendient’s founder and senior partner. “North Carolina is the 9th most populous state today, and it’s projected to be the 7th most populous by the early 2030s, displacing Ohio. We are certainly seeing the impact of population growth in bed need, particularly in fast-growing urban and suburban communities.”
The Acute Care Service Committee recently increased bed needs in some counties, with need determinations now spanning 15 service areas. As of the Sept. 9 meeting, here is where bed needs stand across the state:
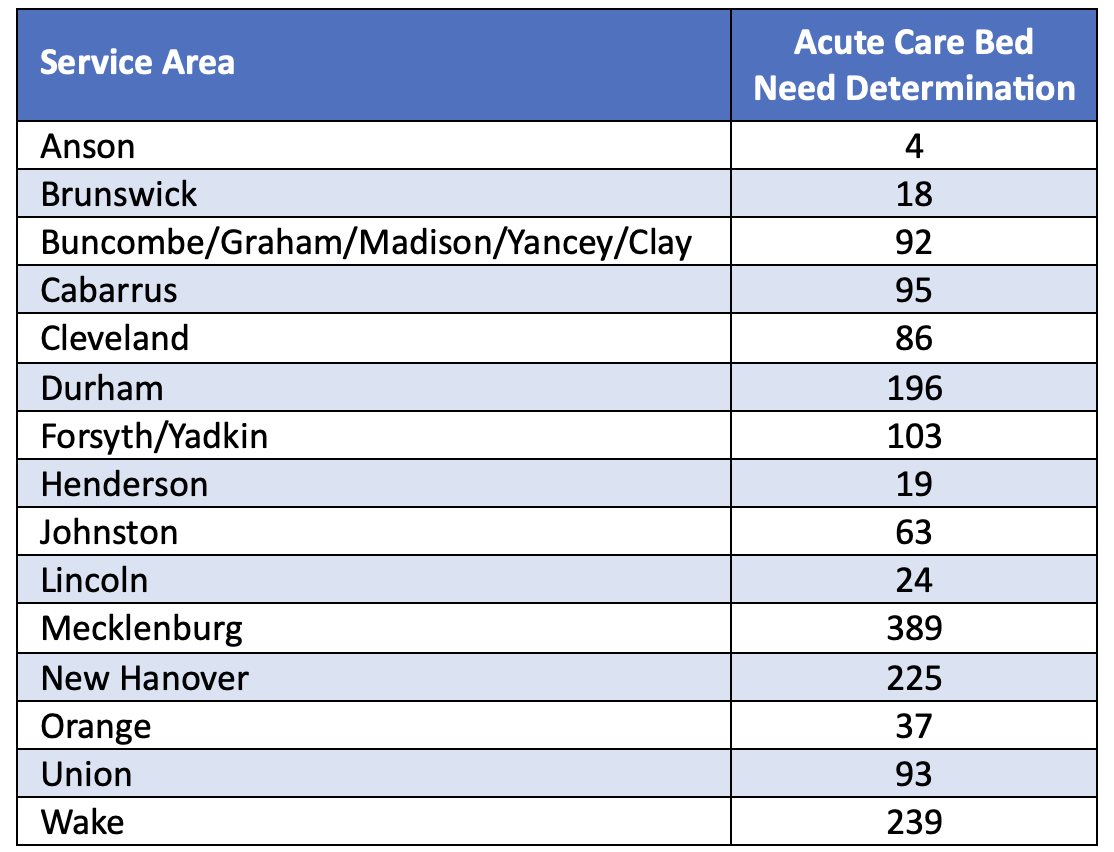
While data updates may continue over the next few weeks, we expect the identified service areas and bed needs in the 2026 SMFP to be set at this point.
Technology and Equipment: A Mixed Picture
Here’s what we’re seeing on the technology and equipment front. No cardiac catheterization or lithotripter needs have emerged in the Plan for 2026. However, a notable cardiac catheterization equipment update worth pointing out is the addition of Policy TE-5 approved by the SHCC earlier this year. Policy TE-5 will allow hospitals operating only one cardiac catheterization unit to apply for a second unit. One caveat to this new policy is that the additional unit may only be used for emergencies and cannot be used for scheduled procedures.
One linear accelerator was identified in the Proposed 2026 SMFP – Service Area 7. Several petitions were filed to add additional linear accelerator needs, with the Technology and Equipment Committee recently recommending approvals for Service Areas 6, 12, and 23. This brings the total to four potential linear accelerator needs – more than we have seen in recent years. A linear accelerator workgroup will begin meeting this fall, with recommendations expected in April 2026.
As for PET imaging, while three fixed PET needs were initially identified in the proposed plan, only two remain following the recent committee meeting: Health Service Areas IV and V. Fixed MRI needs span multiple counties, and an open forum to discuss CON-relevant MRI changes will be held before year-end.
Hospice Home Care: Significant Reductions After Extensive Debate
Perhaps the most dramatic changes involve hospice home care needs. Nine counties were initially identified with hospice home care office need determinations – more than our team has seen in recent memory. However, following extensive petitions and committee discussions, the Long Term and Behavioral Health Committee voted to include only three need determinations for hospice home care: Johnston, McDowell, and Haywood counties.
The committee's rationale centered on COVID-19 impacts and the hospice home care methodology threshold of 90 patients. While only Johnston County exceeded this threshold, the committee acknowledged deficits in Haywood and McDowell Counties based on regional knowledge from committee members. The other six need determinations under consideration were eliminated after considerable debate.
In terms of other post-acute and long-term care needs, two adult care home bed need determinations were in the Proposed 2026 SMFP: Halifax and Perquimans counties. No home health agency/office or inpatient hospice determinations were identified in the proposed plan and a petition for a home health need in Union County was denied.
Regulatory Changes Continue to Evolve
The impact of recent CON deregulation continues to reshape the planning landscape. With qualifying ambulatory surgical facilities (QUASFs) now exempt from CON requirements, the SHCC approved adjustments to the operating room need determination methodology earlier this year.
Operating room need determinations for counties with populations greater than 125,000 will now be for informational purposes only, with the summer petition process available for these counties. Hospital and ASC providers in counties under 125,000 population will not be affected by the methodology changes. No operating room need determinations are in the Proposed 2026 SMFP, and none have emerged during the planning process.
Looking Ahead
The full SHCC meeting on Oct. 1 is where things will be solidified – while committee approvals could theoretically be reversed, we expect the final 2026 SMFP to closely align with recent committee decisions. Following this meeting, the plan will move to the Governor for signature by year-end. We will also look to the schedule of application filing dates to be released in the late November to early December timeframe.
Kim Meymandi contributed research for this post.